ACHAIKI IATRIKI | 2024; 43(2):87-95
Review
Georgios Iliopoulos
Department of Rheumatology, University of Patras Medical School, Patras, Greece
Received: 23 Dec 2023; Accepted: 13 Feb 2024
Corresponding author: Georgios Iliopoulos, Department of Rheumatology, University of Patras Medical School, Patras, Greece, E-mail: geoil22@hotmail.com
Key words: Gout, hyperuricemia, tophi
Abbreviations: NSAIDs, non-steroidal anti-inflammatory drugs; GCs, glucocorticoids; ULT, urate lowering therapy; UA, uric acid.
![]()
Abstract
Gout is a chronic form of inflammatory arthritis characterized by monosodium urate (MSU) crystal deposition in mostly articular but also periarticular structures, such as tendons and bursae. Typically, gout is presented as acute monoarthritis, with self-limiting flares lasting from a few days up to two weeks. Although gout is treatable, 15% of patients can progress to advanced disease, if left untreated. Hyperuricemia, defined as serum uric acid (UA) higher than 6.8mg/dl, is considered the main driver of gout in most cases. Hyperuricemia and therefore MSU crystal formation stems from two broad categories being purine overproduction and decreased UA excretion. Hyperuricemia is usually asymptomatic in the early stage, but frequent gout flares may lead to chronic disease characterized by the presence of tophi, also known as tophaceous gout. Diagnosis can be clinical mostly in cases of podagra, but the gold standard is synovial fluid aspiration from involved joints where applicable. MSU crystal discovery on polarized microscopy yields 100% specificity in gout diagnosis. Gout treatment revolves around two main axons, acute flare management and chronic urate lowering therapy (ULT). Acute flares can be controlled with non-steroidal anti-inflammatory drugs (NSAIDs), colchicine or corticosteroids. The ULT drug of choice is allopurinol, a xanthine oxidase (XO) inhibitor. When ULT is prescribed, concomitant colchicine is administered as gout flare prophylaxis. Therapeutic measures regarding gout patients ought to be individualized, based on gout flare risk and comorbidity burden. In this narrative review we aimed to summarize and enhance the understanding of gout epidemiology, basic pathophysiology features, as well as management and follow-up.
INTRODUCTION
Gout is a chronic form of inflammatory arthritis characterized by monosodium urate (MSU) crystal deposition in mostly articular but also periarticular structures, such as tendons and bursae [1]. Typically, gout is presented as acute monoarthritis, with self-limiting flares lasting from a few days up to two weeks, while peak intensity of pain arises in the first 12 hours. Although gout is treatable, preventable and certainly not life-threatening, 15% of patients can progress to advanced disease (tophi and erosive arthritis), if left untreated [2]. In this narrative review, we aimed to summarize and enhance the understanding of gout epidemiology, basic pathophysiology features, as well as management and follow-up.
MATERIALS AND METHODS
We conducted an electronic data search on Medline and Scopus from inception until November 2023. We used the keyword “gout” in combination with “hyperuricemia, clinical presentation, treatment” and assessed all articles. The inclusion criteria were that articles should derive from clinical trials, reviews or meta-analyses and should be written in English. Exclusion criteria were sporadic case reports with peculiar or atypical forms of gout. All in all, we chose the most representative and high-impact articles that served the purpose of this narrative review.
EPIDEMIOLOGY AND RISK FACTORS
Hyperuricemia is considered the main driver of gout in most cases. According to the definition of hyperuricemia, blood serum uric acid (UA) exceeds 6.8 mg/dl, which surpasses the point of MSU solubility threshold and subsequently MSU crystallization occurs [3]. Hyperuricemia is very common with a prevalence of 20% approximately [4]. However, according to recent data, less than 50% of those with UA over 10mg/dl will develop a gout attack throughout a 10–15-year period [5]. Consequently, although hyperuricemia is necessary for gout development, people with asymptomatic hyperuricemia may never develop gout. While gout epidemiology varies among different ethnic groups, 4-6% of the population suffer from this disease [6], whereas incidence revolves around 1-3 per thousand person-years [7]. Gout is most common in older males and the most prevalent risk factor is a purine-rich diet, especially excess alcohol consumption with a great emphasis on beer [8]. High purine diets include shellfish and red meat amongst others. Gout was known in the past as the “disease of kings” because if anyone could afford to eat a steak and accompany it with an alcoholic beverage, then he must have been a king [9]. Other renown risk factors include men over the age of 40 and post-menopausal women, smoking, family history (heritability of hyperuricemia up to 60%) [10] and comorbidities like chronic kidney disease (CKD), metabolic syndrome, thyroid dysfunction, diabetes and certain medication, such as diuretics, beta-blockers and aspirin (mainly low dose) [11]. However, a recent mendelian study failed to prove a clear association between alcohol consumption and gout development [12]. Taken together, these data question the role of environmental risk factors in gout incidence.
ETIOLOGY AND PATHOPHYSIOLOGY
Purine overproduction and decreased UA excretion are the 2 main mechanisms leading to hyperuricemia and subsequent MSU crystal formation [5]. MSU crystals are formed because the solubility threshold of monosodium urate (6.8 mg/dl) is exceeded. Hematologic malignancies, metabolic syndrome, psoriasis, cytotoxic drugs and substances, especially alcohol can lead to purine overproduction. On the other hand, decreased UA excretion can be noted in several situations as in metabolic acidosis, CKD and volume depletion conditions. It is established that transmembrane transporters in the proximal renal tubule dictate UA excretion [13]. Many transporters have been described, the most common being ATP binding cassette G2 (ABCG2), Glucose transporter 9 (GLUT9), urate transporter 1 (URAT1) and organic anion transporters (OAT). Latest research revealed the role of gut in UA excretion [14]. Increase of harmful bacteria, namely Prevotella and Bacteroides species and the decrease of protective ones, such as Enterobacteriaceae and Faecalibacterium species, leads to increase UA production and decreased kidney and intestine UA excretion, resulting in hyperuricemia and possibly facilitating gout flares. Enterocytes have been proven to express similar transporters that facilitate UA transfer. ABCG2 is a shared transporter of both gut and renal tubules. Mutations and polymorphisms in those transporters have been associated with hyperuricemia and can lead to impaired UA handling by the kidney [15]. Although gout pathophysiology is not entirely clear, innate immunity is considered the main driver of associated inflammatory responses [16]. Macrophages express Toll-Like Receptors (TLRs) on their surface, which recognize MSU crystals in the form of danger-associated molecular patterns. Then, MSU crystals are phagocytosed leading to upregulation of proinflammatory pathways such as nuclear factor kappa B (NF-κB) pathway and NOD-Like Receptor 3 (NLRP3) inflammasome is constructed leading to caspase 1 production. Then, caspase cleaves pro-IL1b to its active form, IL-1b. This cytokine in turn orchestrates the inflammatory response through endothelium activation and neutrophil recruitment with neutrophils being the main offenders of gout flare [17]. As stated above, gout flares are self-limited and usually resolve within a few days. This is possible because even though neutrophils drive gout inflammation, they are also capable of stopping it. They excrete their DNA content, known as neutrophil extracellular traps (NETs), which bind MSU crystals and along with concomitant production anti-inflammatory cytokines, mostly IL-10 and TGF-β lead to flare resolution [18].
CLINICAL CHARACTERISTICS
A typical gout attack usually involves the 1st metatarsophalangeal joint (MTP) and in this case it is called podagra [19]. Monoarthritis is the most frequent presentation, but oligoarthritis (2-4 joints) is not uncommon, whereas polyarthritis is rare. Other commonly involved joints include the knees, ankles, wrists and other MTP and finger joints [20]. The attacks are self-remitting within a few days and the peak pain intensity occurs in the first hours. Clinical presentation encompasses all the textbook signs of inflammation such as redness, swelling, warmth and great sensitivity to touch [21]. Lab tests can reveal elevated inflammatory markers, leukocytosis and sometimes the patient may complain of fever and malaise. Recurrent gout flares can lead to chronic disease called tophaceous gout identified by tophi formation [22]. Tophi are subcutaneous nodules made of MSU crystals. The most frequent sites of tophi deposition are the ears [23], elbows, small joints of the hands and feet. Except for the aesthetic aspect, tophi can be dangerous if left untreated without proper urate lowering therapy (ULT) and monitoring. They can cause bone erosions, structural joint damage and can become infected [24].
EVALUATION AND DIFFERENTIAL DIAGNOSIS
When evaluating an acute monoarthritis, one must contemplate that although gout necessitates hyperuricemia, serum UA is of extremely low specificity in gout for 2 reasons [25]. Firstly, during a gout flare and inflammation in general, serum UA might be falsely normal or even decreased [26]. Secondly, individuals with hyperuricemia may never suffer a gout attack. Diagnosis can be clinical mostly in cases of podagra, but the gold standard is synovial fluid aspiration from involved joints where applicable [27]. This is especially true for large joints, the most prominent being the knees and elbows. MSU crystal discovery on polarized microscopy yields 100% specificity in gout diagnosis. Negative birefringence is characteristic of gout, where needle-shaped crystals appear yellow when parallel to polarized light axis [28]. They should not be confused with Calcium Pyrophosphate Dihydrate Deposition Disease (CPPD) crystals, which have a rhomboid appearance and have positive birefringence, appearing blue when parallel to the polarized light axis. That being said, perhaps the greatest utility of joint aspiration is the exclusion of septic arthritis, a potent gout mimic with high mortality [29]. Septic arthritis occurs when a pathogen, usually bacteria, invades and assaults the joint microenvironment. Most common pathogens in fluid culture include Staphylococcus Aureus, Neisseria gonorrhoeae and streptococcal species. Fluid analysis typically reveals a white blood cell (WBC) count of over 50,000 cells with a Polymorphonuclear Neutrophil (PMN) predominance of over 75%. Treatment approach in septic arthritis is a far cry from gout [30]. Measures encompass joint immobilization, percutaneous fluid drainage and empirical administration of wide spectrum antibiotics until culture results are available [31]. Rarely, septic arthritis can coexist with gout, as described in several case reports [32]. The most involved joint is the knee. Synovial fluid aspiration is important in such cases because the presence of high cell count (>50000 cells) along with concomitant fever and remarkably high inflammatory markers, may alert physicians towards septic arthritis coexistence. Other gout mimics include CPPD arthropathy, also known as pseudogout, meaning “false” gout, indicating similarities in both entities. Both are characterized by monoarthritis (for the most part) due to crystal deposition [33]. However, CPPD arthropathy is regularly associated with hyperparathyroidism, hypomagnesemia, CKD and hypothyroidism and predominantly affects elderly patients. Other systemic rheumatic diseases (RMDs), for instance rheumatoid arthritis (RA) or psoriatic arthritis (PsA), can showcase similar clinical presentation to gout [34]. The key differential diagnostic feature in this case is the acuteness of onset. Gout presents with an acute and sudden onset, whereas RMDs unravel joint-related symptoms gradually. Notably, psoriasis and PsA patients have a higher risk of developing gout compared to the general population [35]. Gout differential diagnosis is summarized concisely in Table 1.
Radiologic tests, although not mandatory for diagnosis, have their utility in patients with mono- or oligo-arthritis [36]. Plain X-rays are often performed mainly for differential diagnostic purposes and not for gout diagnosis per se. For example, when history of trauma is present, X-rays may reveal a fracture or when CPPD is suspected, chondrocalcinosis of the involved joint may be observed. Furthermore, X-rays can confirm tophi, which are radio-opaque due to calcification [37]. Erosions can also be noted, especially in chronic tophaceous gout, giving the appearance of “overhanging edges”, a sign resulting from disruption of the outer bone cortex. Wherever available, ultrasound (U/S) of the involved area may reveal the double contour sign resulting from MSU crystal deposition on hyaline cartilage, which is unique to gout [38]. Dual-energy computed tomography (CT) can provide useful information in patients with chronic gout, as MSU crystals can deposit in periarticular tissues [39], even in peculiar places like the spine [40]. It is a specific CT sequence, where MSU crystals appear in green color most of the time [41]. Cases of low-back pain have been attributed to gout after performing dual-energy CT, which uncovered MSU crystals accumulating in the spine. However, higher cost dictates that dual-energy CT should be used sparingly [42].
TREATMENT AND FOLLOW-UP
Gout treatment revolves around three main axons, non-steroidal anti-inflammatory drugs (NSAIDs), corticosteroids (CS) and colchicine [43]. One therapeutic measure is not necessarily better than the other and physicians should follow an individualized approach [44]. NSAIDs, albeit a valid option for younger relatively healthy individuals, should be avoided in patients with many comorbidities, most notably cardiovascular disease (CVD) or CKD [45,46]. If NSAIDs are chosen as the drug of choice though, their full anti-inflammatory dose should be prescribed for one week approximately and not just symptomatic treatment [47]. CS, at a dose of 0.5mg/kg of bodyweight, can be effective for treating gout flare. Parenteral CS can possibly lead to faster flare resolution and constitute a more practical approach as they can be administered intramuscularly (IM) in the form of betamethasone or triamcinolone once or twice throughout the gout attack [48]. Nonetheless, patients with uncontrolled or poorly monitored diabetes should avoid CS [49]. Colchicine remains the cornerstone of gout flare treatment and prophylaxis [50]. When choosing to use colchicine, a tablet of 1mg must be administered at the time of gout flare diagnosis and 0.5mg 1 hour after the first pill. Then, 0.5mg can be given once or twice daily for a week or longer if prophylactic therapy is needed. In that case, colchicine should be prescribed as prophylaxis along ULT until the target of serum UA below 6mg/dl is reached and the patient is without flare for at least 1 month [51]. Recently, we have proven that IM tetracosactide, an ACTH analogue, showed favorable therapeutic outcomes in hospitalized patients with gout [52]. That should come as no surprise, since ACTH as a drug is approved by the Food and Drug Administration (FDA) in gout [53]. Except for cortisol production mobilization, the mechanism of action of tetracosactide pertains to a potent anti-inflammatory effect stemming from melanocortin receptor (MCR) binding, especially MC3R. The cortisol produced, along with the anti-inflammatory action of tetracosactide, makes this agent a plausible alternative to GCs. Anakinra, an IL-1 receptor antagonist, administered subcutaneously (SC) at a dose of 100mg daily, can be reserved for severe gout flares in patients with heavy comorbidity burden, which does not allow for the usual therapeutic agents [54]. Albeit effective for gout flares, anakinra should be used sparingly due to high cost-to-benefit ratio. Canakinumab, a selective IL-1β blocker, constitutes another potent therapeutic option in severe gout [55]. Nevertheless, canakinumab is directed towards special cases due to high cost.
Once gout flare is resolved, decisions regarding hyperuricemia must be made. All patients with even one gout attack in their lifetime should be assessed for comorbidities creating a hyperuricemic environment, especially cardiometabolic disease. Nevertheless, patients with very sporadic gout attacks may not need ULT [56]. However, more than two flares per year and the presence of tophi or erosions necessitates ULT. The ULT drug of choice is allopurinol, a xanthine oxidase (XO) inhibitor [57]. An initial dose of 100mg is administered and serum UA must be measured every three to six weeks until target serum UA is reached. According to consensus and recommendations, the target is 6mg/dl and allopurinol dosage can be escalated up to 800mg daily to achieve this goal [58]. In the case of tophaceous arthritis, the target UA threshold is lowered to 5mg/dl [47]. Also, due to the destructive nature of tophi and their erosive potential, ULT tends to require closer monitoring. When ULT is prescribed, concomitant colchicine is administered as gout flare prophylaxis until target serum UA is reached and the patient is free of flares for at least 1 month [59]. The rationale behind colchicine prophylaxis revolves around the hypothesis of MSU crystal mobilization from periarticular structures following ULT that can trigger local immune responses inflicting a gout flare. Colchicine as prophylaxis is usually administered at the dose of 0.5mg daily or bidaily. Second line ULT agents encompass febuxostat [60], another XO inhibitor, which is prescribed in cases of allopurinol allergic reaction or intolerance. Another ULT class, uricosurics, especially probenecid can be useful in treating gout in patients who cannot tolerate a XO inhibitor, but extra attention should be warranted towards the patient having adequate liquid daily intake due to high risk of renal stone formation [61]. That being said, uricosurics have been combined with XO inhibitors with success regarding serum UA lowering compared to monotherapy [62]. In extreme case of gout and tophaceous arthritis where all therapeutic approaches have failed, pegloticase, a recombinant uricase, can be administered with biweekly intravenous (IV) infusions, but physicians must be aware of two possible hazards [63]. The first is the development of antidrug autoantibodies and the second is the high risk of infusion reaction. To avoid both situations, concomitant immunosuppressive therapy is recommended from the start and the agents of choice are methotrexate and mycophenolate mofetil (MMF). Figure 1 outlines a therapeutic approach algorithm for gout patients.
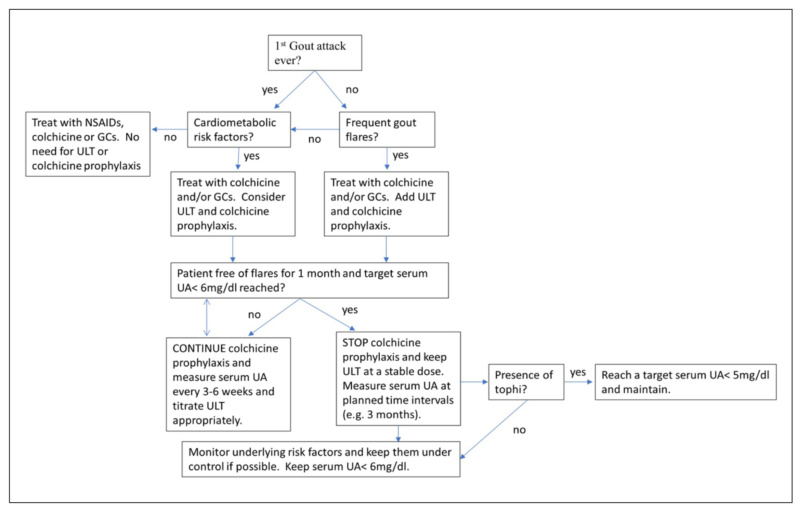
Figure 1. Gout Therapeutic Approach Algorithm.
Finally, the urate-lowering potential of lifestyle modifications has been a matter of controversy over the years [25]. Often, patients prefer to try and modify their daily habits rather than taking ULT medication. Although alcohol cessation (and especially beer) is essential to avoiding gout flares, lifestyle modifications have been proven to have modest benefit at best [64]. That is not to say that patients should deviate from healthy eating, fat loss (where applicable) and comorbidities management, but one should not hope for a meaningful change in serum UA with lifestyle changes alone [65]. Maybe the best practice is reflected by a combination of ULT and daily habits alterations [66].
SPECIAL CONSIDERATIONS
In everyday clinical practice, there is a trend towards treating asymptomatic hyperuricemia without gout history [67]. Despite the rationale behind this practice, the benefit of ULT is not guaranteed to outweigh the cost, namely drug reactions [68], adverse events and interactions [69]. According to a meta analysis, patients with serum UA values higher than 10mg/dl had less than 50% chance of suffering a gout attack in 15 years, whereas the incidence at five-year-period was approximately 25% [70]. Of course, there is a time for exceptions and risk stratification, particularly in patients with metabolic syndrome, CKD or CVD, where hyperuricemia could act as a secondary cardiovascular risk factor [57]. Another important consideration is patient education regarding gout attack management [71]. Towards this direction, the “pill-in-a-pocket” approach has been proposed [72]. According to this method, the patient is literally prepared to face a gout flare, by having tablets of colchicine, corticosteroids or NSAIDs, readily available, ensuring timely intervention and a potentially faster flare resolution. Another topic of concern seems to be the place of allopurinol in CKD patients. Physicians are oftentimes reluctant to prescribe ULT therapy in such cases, confusing allopurinol with colchicine. Indeed, colchicine should be used cautiously in patients with estimated glomerular filtration rate (eGFR) lower than 30 ml/min. Wei et al found no worsening of renal function or reduced survival in moderate to severe CKD patients who took allopurinol [73]. With that in mind, CKD patients were found to have increased risk of allopurinol hypersensitivity reaction [74]. This is particularly true for people who are positive for a specific human leukocyte antigen (HLA), HLA-B*5801, commonly encountered in Asian and African American populations [75]. Allopurinol hypersensitivity reaction is characterized by diffuse rash, acute kidney or hepatic injury and high blood eosinophil count, usually in the context of drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome [76]. In the event of such a reaction, topical or systemic corticosteroids should be administered, following immediate allopurinol cessation. Another topic reserved for last is the heart involvement in patients receiving febuxostat treatment. According to the 2018 CARES trial [77], increased CVD-related and all-cause mortality was noticed in the febuxostat versus allopurinol group, following randomization. This observation even led the FDA to issue a febuxostat black box warning for CVD patients. However, those findings were not replicated in the 2020 FAST trial [78], where no difference in CVD events or death were noted between the two groups. Results should be always taken with a grain of salt, since CARES trial had 50% loss to follow-up compared with 5.8% of the FAST trial. All in all, febuxostat appears to be safe in patients with heart involvement.
CONCLUSION
Gout management, albeit seemingly simple, requires a multifactorial and multidisciplinary approach. Frequent gout flares render ULT unavoidable, while lifestyle changes have modest benefits. Nevertheless, patient education remains crucial [79]. In any case, therapeutic approach plans for gout patients ought to be individualized, based on gout flare risk and comorbidity burden [80].
Conflict of interest disclosure
None to declare
Declaration of funding sources
None to declare
Author contributions
George Iliopoulos is the sole author, and he has read and agreed to the published version of the manuscript.
REFERENCES
- Dalbeth N, Merriman TR, Stamp LK. Gout. Lancet (London, England). 2016;388(10055):2039–52.
- Brook RA, Forsythe A, Smeeding JE, Lawrence Edwards N. Chronic gout: epidemiology, disease progression, treatment and disease burden. Curr Med Res Opin. 2010;26(12):2813–21.
- Yanai H, Adachi H, Hakoshima M, Katsuyama H. Molecular Biological and Clinical Understanding of the Pathophysiology and Treatments of Hyperuricemia and Its Association with Metabolic Syndrome, Cardiovascular Diseases and Chronic Kidney Disease. Int J Mol Sci. 2021;22(17).
- He H, Guo P, He J, Zhang J, Niu Y, Chen S, et al. Prevalence of hyperuricemia and the population attributable fraction of modifiable risk factors: Evidence from a general population cohort in China. Front Public Heal. 2022;10:936717.
- Fenando A, Rednam M, Gujarathi R, Widrich J. Gout. [Updated 2022 Dec 27]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK546606/
- Pentyala S, Monastero R, Palati S, Varghese E, Anugu A, Pentyala S, et al. Rapid Gout Detection Method and Kit. Diagnostics (Basel, Switzerland). 2019;9(4):157.
- Abhishek A, Roddy E, Doherty M. Gout – a guide for the general and acute physicians. Clin Med. 2017;17(1):54–9.
- Helget LN, Mikuls TR. Environmental Triggers of Hyperuricemia and Gout. Rheum Dis Clin North Am. 2022;48(4):891–906.
- Tang SCW. Gout: A Disease of Kings. Contrib Nephrol. 2018;192:77–81.
- Major TJ, Dalbeth N, Stahl EA, Merriman TR. An update on the genetics of hyperuricaemia and gout. Nat Rev Rheumatol. 2018;14(6):351–3.
- Dehlin M, Jacobsson L, Roddy E. Global epidemiology of gout: prevalence, incidence, treatment patterns and risk factors. Nat Rev Rheumatol. 2020;16(7):380–90.
- Syed AAS, Fahira A, Yang Q, Chen J, Li Z, Chen H, et al. The Relationship between Alcohol Consumption and Gout: A Mendelian Randomization Study. Genes (Basel). 2022;13(4):557.
- Torres RJ, Puig JG. GLUT9 influences uric acid concentration in patients with Lesch-Nyhan disease. Int J Rheum Dis. 2018;21(6):1270–6.
- Tong S, Zhang P, Cheng Q, Chen M, Chen X, Wang Z, et al. The role of gut microbiota in gout: Is gut microbiota a potential target for gout treatment. Front Cell Infect Microbiol. 2022 24;12:1051682.
- Clavijo-Cornejo D, Hernández-González O, Gutierrez M. The current role of NLRP3 inflammasome polymorphism in gout susceptibility. Int J Rheum Dis. 2021;24(10):1257–65.
- Dalbeth N, Gosling AL, Gaffo A, Abhishek A. Gout. Lancet (London, England). 2021;397(10287):1843–55.
- Liu W, Peng J, Wu Y, Ye Z, Zong Z, Wu R, et al. Immune and inflammatory mechanisms and therapeutic targets of gout: An update. Int Immunopharmacol. 2023;121:110466.
- Dalbeth N, Choi HK, Joosten LAB, Khanna PP, Matsuo H, Perez-Ruiz F, et al. Gout. Nat Rev Dis Prim. 2019;5(1):69.
- Stewart S, Dalbeth N, Vandal AC, Rome K. The first metatarsophalangeal joint in gout: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2016;17(1):69.
- Richette P, Doherty M, Pascual E, Barskova V, Becce F, Castañeda-Sanabria J, et al. 2016 updated EULAR evidence-based recommendations for the management of gout. Ann Rheum Dis. 2017;76(1):29–42.
- Perez-Ruiz F, Castillo E, Chinchilla SP, Herrero-Beites AM. Clinical manifestations and diagnosis of gout. Rheum Dis Clin North Am. 2014;40(2):193–206.
- Sun C, Qi X, Tian Y, Gao L, Jin H, Guo H. Risk factors for the formation of double-contour sign and tophi in gout. J Orthop Surg Res. 2019;14(1):239.
- Saliba J, Sakano H, Friedman RA, Harris JP. Tophaceous gout of the middle ear: Case reports and review of the literature. Audiol Neurotol. 2019;24(2):51–5.
- Kumar S, Aggarwal D, Mehta H, De D, Handa S, Radotra BD. Gouty tophi. J community Hosp Intern Med Perspect. 2014;4(1):182.
- Gwinnutt JM, Wieczorek M, Balanescu A, Bischoff-Ferrari HA, Boonen A, Cavalli G, et al. 2021 EULAR recommendations regarding lifestyle behaviours and work participation to prevent progression of rheumatic and musculoskeletal diseases. Ann Rheum Dis. 2023;82(1):48–56.
- Zhang J, Sun W, Gao F, Lu J, Li K, Xu Y, et al. Changes of serum uric acid level during acute gout flare and related factors. Front Endocrinol (Lausanne). 2023;14:1077059.
- Richette P, Doherty M, Pascual E, Barskova V, Becce F, Castaneda J, et al. 2018 updated European League Against Rheumatism evidence-based recommendations for the diagnosis of gout. Ann Rheum Dis. 2020;79(1):31–8.
- Zhang Y, Lee SYC, Zhang Y, Furst D, Fitzgerald J, Ozcan A. Wide-field imaging of birefringent synovial fluid crystals using lens-free polarized microscopy for gout diagnosis. Sci Rep. 2016;6:28793..
- Clebak KT, Morrison A, Croad JR. Gout: Rapid Evidence Review. Am Fam Physician. 2020;102(9):533–8.
- García-Arias M, Balsa A, Mola EM. Septic arthritis. Best Pract Res Clin Rheumatol. 2011;25(3):407–21.
- Ross JJ. Septic Arthritis of Native Joints. Infect Dis Clin North Am. 2017;31(2):203–18.
- Yu KH, Luo SF, Liou LB, Wu YJJ, Tsai WP, Chen JY, et al. Concomitant septic and gouty arthritis—an analysis of 30 cases. Rheumatology. 2003;42(9):1062–6.
- Schlee S, Bollheimer LC, Bertsch T, Sieber CC, Härle P. Crystal arthritides – gout and calcium pyrophosphate arthritis : Part 2: clinical features, diagnosis and differential diagnostics. Z Gerontol Geriatr. 2018;51(5):579–84.
- Zamora EA, Naik R. Calcium Pyrophosphate Deposition Disease. [Updated 2023 Jun 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK540151/
- Wei JCC, Chang YJ, Wang YH, Yeh CJ. The Risk of Gout in Patients with Psoriasis: A Population-Based Cohort Study in Taiwan. Clin Epidemiol. 2022;14:265.
- Sudoł-Szopińska I, Afonso PD, Jacobson JA, Teh J. Imaging of gout: findings and pitfalls. A pictorial review – PubMed. Acta Reumatol Port. 2020 J;45(1):20-5.
- Araujo EG, Manger B, Perez-Ruiz F, Thiele RG. Imaging of gout: New tools and biomarkers? Best Pract Res Clin Rheumatol. 2016;30(4):638–52.
- Zhang B, Yang M, Wang H. Diagnostic value of ultrasound versus dual-energy computed tomography in patients with different stages of acute gouty arthritis. Clin Rheumatol. 2020;39(5):1649–53.
- Andia I, Abate M. Hyperuricemia in Tendons. Adv Exp Med Biol. 2016;920:123–32.
- Chen HJ, Chen DY, Zhou SZ, Chi K De, Wu JZ, Huang FL. Multiple tophi deposits in the spine: A case report. World J Clin cases. 2022;10(29):10647–54.
- Khanna I, Pietro R, Ali Y. What Has Dual Energy CT Taught Us About Gout? Curr Rheumatol Rep. 2021;23(9):71.
- Ahn SJ, Zhang D, Levine BD, Dalbeth N, Pool B, Ranganath VK, et al. Limitations of dual-energy CT in the detection of monosodium urate deposition in dense liquid tophi and calcified tophi. Skeletal Radiol. 2021;50(8):1667–75.
- Pillinger MH, Mandell BF. Therapeutic approaches in the treatment of gout. Semin Arthritis Rheum. 2020;50(3S):S24–30.
- Yu J, Lu H, Zhou J, Xie Z, Wen C, Xu Z. Oral prednisolone versus non-steroidal anti-inflammatory drugs in the treatment of acute gout: a meta-analysis of randomized controlled trials. Inflammopharmacology. 2018;26(3):717–23.
- Baker M, Perazella MA. NSAIDs in CKD: Are They Safe? Am J Kidney Dis. 2020;76(4):546–57.
- Ghosh R, Alajbegovic A, Gomes A V. NSAIDs and Cardiovascular Diseases: Role of Reactive Oxygen Species. Oxid Med Cell Longev. 2015;2015:536962.
- FitzGerald JD, Dalbeth N, Mikuls T, Brignardello-Petersen R, Guyatt G, Abeles AM, et al. 2020 American College of Rheumatology Guideline for the Management of Gout. Arthritis Rheumatol (Hoboken, NJ). 2020;72(6):879–95.
- Liu X, Sun D, Ma X, Li C, Ying J, Yan Y. Benefit-risk of corticosteroids in acute gout patients: An updated meta-analysis and economic evaluation. Steroids. 2017;128:89–94.
- Elena C, Chiara M, Angelica B, Chiara MA, Laura N, Chiara C, et al. Hyperglycemia and Diabetes Induced by Glucocorticoids in Nondiabetic and Diabetic Patients: Revision of Literature and Personal Considerations. Curr Pharm Biotechnol. 2018;19(15):1210–20.
- Pascart T, Richette P. Colchicine in Gout: An Update. Curr Pharm Des. 2018;24(6):684–9.
- Latourte A, Bardin T, Richette P. Prophylaxis for acute gout flares after initiation of urate-lowering therapy. Rheumatol (United Kingdom). 2014;53(11):1920–6.
- Daoussis D, Kordas P, Varelas G, Michalaki M, Onoufriou A, Mamali I, et al. ACTH vs steroids for the treatment of acute gout in hospitalized patients: a randomized, open label, comparative study. Rheumatol Int. 2022;42(6):949–58.
- Iliopoulos G, Daoussis D. FDA-Approved indications of adrenocorticotropic hormone (ACTH) as a drug: Does it have a place in disease management today? Cent Asian J Med Hypotheses Ethics. 2022;3(4):220–31.
- Saag KG, Khanna PP, Keenan RT, Ohlman S, Osterling Koskinen L, Sparve E, et al. A Randomized, Phase II Study Evaluating the Efficacy and Safety of Anakinra in the Treatment of Gout Flares. Arthritis Rheumatol (Hoboken, NJ). 2021;73(8):1533–42.
- Schlesinger N. Canakinumab in gout. Expert Opin Biol Ther. 2012;12(9):1265–75.
- Perez-Gomez MV, Bartsch LA, Castillo-Rodriguez E, Fernandez-Prado R, Kanbay M, Ortiz A. Potential Dangers of Serum Urate-Lowering Therapy. Am J Med. 2019;132(4):457–67.
- Kutzing MK, Firestein BL. Altered uric acid levels and disease states. J Pharmacol Exp Ther. 2008;324(1):1–7.
- Perez-Ruiz F, Dalbeth N. Gout. Rheum Dis Clin North Am. 2019;45(4):583–91.
- Afinogenova Y, Danve A, Neogi T. Update on gout management: what is old and what is new. Curr Opin Rheumatol. 2022;34(2):118–24.
- Bardin T, Richette P. The role of febuxostat in gout. Curr Opin Rheumatol. 2019;31(2):152–8.
- Probenecid – PubMed [Internet]. [cited 2023 Dec 22]. Available from: https://pubmed.ncbi.nlm.nih.gov/31643913/
- Perez-Ruiz F, Dalbeth N. Combination urate-lowering therapy in the treatment of gout: What is the evidence? Semin Arthritis Rheum. 2019;48(4):658–68.
- Drugs and Lactation Database (LactMed®) [Internet]. Bethesda (MD): National Institute of Child Health and Human Development; 2006-. Pegloticase. [Updated 2023 Nov 15]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK573040/
- Danve A, Sehra ST, Neogi T. Role of diet in hyperuricemia and gout. Best Pract Res Clin Rheumatol. 2021;35(4):101723.
- Bai L, Zhou J-B, Zhou T, Newson RB, Cardoso MA. Incident gout and weight change patterns: a retrospective cohort study of US adults. Arthritis Res Ther. 2021;23(1):69.
- Ashiq K, Bajwa MA, Tanveer S, Qayyum M, Ashiq S, Khokhar R, et al. A comprehensive review on gout: The epidemiological trends, pathophysiology, clinical presentation, diagnosis and treatment. J Pak Med Assoc. 2021;71(4):1234–8.
- Yip K, Cohen RE, Pillinger MH. Asymptomatic hyperuricemia: is it really asymptomatic? Curr Opin Rheumatol. 2020;32(1):71–9.
- Shi C, Zhou Z, Chi X, Xiu S, Yi C, Jiang Z, et al. Recent advances in gout drugs. Eur J Med Chem. 2023;245(Pt 1).
- Lorenzo JPP, Sollano MHMZ, Salido EO, Li-Yu J, Tankeh-Torres SA, Wulansari Manuaba IAR, et al. 2021 Asia-Pacific League of Associations for Rheumatology clinical practice guideline for treatment of gout. Int J Rheum Dis. 2022;25(1):7–20.
- Dalbeth N, Phipps-Green A, Frampton C, Neogi T, Taylor WJ, Merriman TR. Relationship between serum urate concentration and clinically evident incident gout: an individual participant data analysis. Ann Rheum Dis. 2018;77(7):1048–52.
- Doherty M, Jenkins W, Richardson H, Sarmanova A, Abhishek A, Ashton D, et al. Efficacy and cost-effectiveness of nurse-led care involving education and engagement of patients and a treat-to-target urate-lowering strategy versus usual care for gout: a randomised controlled trial. Lancet (London, England). 2018;392(10156):1403–12.
- Richette P, Bardin T. Colchicine for the treatment of gout. Expert Opin Pharmacother. 2010;11(17):2933–8.
- Wei J, Choi HK, Neogi T, Dalbeth N, Terkeltaub R, Stamp LK, et al. Allopurinol Initiation and All-Cause Mortality Among Patients With Gout and Concurrent Chronic Kidney Disease : A Population-Based Cohort Study. Ann Intern Med. 2022;175(4):461–70.
- Bathini L, Garg AX, Sontrop JM, Weir MA, Blake PG, Dixon SN, et al. Initiation Dose of Allopurinol and the Risk of Severe Cutaneous Reactions in Older Adults With CKD: A Population-Based Cohort Study. Am J Kidney Dis. 2022;80(6):730–9.
- Park DJ, Kang JH, Lee JW, Lee KE, Wen L, Kim TJ, et al. Cost-effectiveness analysis of HLA-B5801 genotyping in the treatment of gout patients with chronic renal insufficiency in Korea. Arthritis Care Res (Hoboken). 2015;67(2):280–7.
- Hama N, Abe R, Gibson A, Phillips EJ. Drug-Induced Hypersensitivity Syndrome (DIHS)/Drug Reaction With Eosinophilia and Systemic Symptoms (DRESS): Clinical Features and Pathogenesis. J allergy Clin Immunol Pract. 2022;10(5):1155-1167.e5.
- White WB, Saag KG, Becker MA, Borer JS, Gorelick PB, Whelton A, et al. Cardiovascular Safety of Febuxostat or Allopurinol in Patients with Gout. N Engl J Med. 2018;378(13):1200-10.
- Mackenzie IS, Ford I, Nuki G, Hallas J, Hawkey CJ, Webster J, et al. Long-term cardiovascular safety of febuxostat compared with allopurinol in patients with gout (FAST): a multicentre, prospective, randomised, open-label, non-inferiority trial. Lancet (London, England). 2020;396(10264):1745–57.
- Abhishek A, Doherty M. Education and non-pharmacological approaches for gout. Rheumatology (Oxford). 2018;57(suppl_1):i51–8.
- Mikuls TR. Gout. Williams WW, Solomon CG, editors. N Engl J Med. 2022;387(20):1877–87.