ACHAIKI IATRIKI | 2020; 39(1): 45–46
Case Report
Christos Konstantakis¹, Spyros Spyropoulos², Vasileios Margaritis²
1Department of Gastroenterology, University Hospital of Patras, 26504 Patras, Greece,
2Department of Gastroenterology, General Hospital of Patras, 26335 Patras, Greece
Received: 07 March 2020; Accepted: 10 March 2020
Corresponding author: Christos Konstantakis, MD, University Hospital of Patras, D. Stamatopoulou 4, Rio 26504, Patras, Greece. Tel.: +30-6974563157, Fax: +30-261-0999518, E mail: asraiah@yahoo.com
Key words: Abdominal pain; foreign body, endoscopic removal, biliary enteric anastomosis
![]()
Abstract
An 82-year-old woman was referred to our hospital because of generalized weakness and vertigo, accompanied by epigastric pain. She complained of progressively worsening shortness of breath on light exertion during the last month. She also reported frequent episodes of (non – debilitating) epigastric pain / discomfort that impacted on her quality of life. The abdominal symptoms varied in frequency and severity but had grown progressively more frequent and severe in the last several months (at least 4 months). Her caretaker (daughter of patient) that provided patient history information reported a complicated cholecystectomy (for gallbladder stone disease) more than 25 years ago and atrial fibrillation (AFib) on dabigatran. Findings from physical examination were mostly nonspecific: Non-tender non-firm smooth hepatomegaly (1-2cm), a systolic 3/6 (functional) murmur and mild epigastric tenderness on deep palpation (Murphy’s, McBurney and Rovsing’s sign negative). Digital rectal examination was also unremarkable. The patient appeared pale, non-icteric and afebrile. The only interesting finding was the scar from an “extended’’ Kocher incision to the abdomen. Initial laboratory examinations revealed decreased hematocrit (26,5 %), hemoglobin levels with depleted iron supplies (low levels MCV, MCH, iron and Ferritin), while the rest of the blood exams (including amylase, bilirubin, liver function tests) appeared unremarkable. An ultrasonographic examination of the abdomen, only managed to confirm the cholecystectomy. The patient was hospitalized, transfused and was administered intravenous iron supplementation. An esophagogastroduodenoscopy (EGD) was ordered, based on chief complains. Findings from the stomach were unremarkable during the EGD. However, inspection of the duodenum bulb revealed a diverticulum – like “pocket’’ with bile coming out of the orifice. On further examination, this was confirmed to be the opening of a biliary enteric anastomosis (BEA). What was also interesting was that inside the distal end of the BEA we found a long chicken bone (Figure 1), which was retrieved with the use of grasping forceps (Figure 2). The patient was shortly after discharged with instructions for further investigation (of anemia). On follow – up, more than 8 weeks later, patient disclosed complete resolution of epigastric symptoms.

Figure 1. Endoscopic imaging of the biliary enteric anastomosis located in the duodenum of the patient. A long foreign body is easily identified
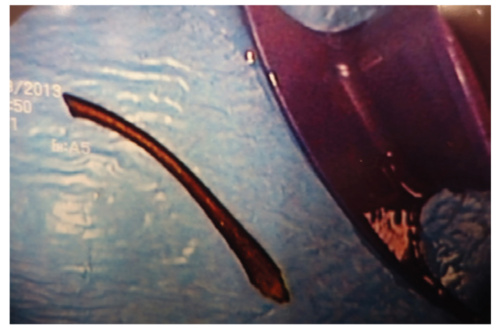
Figure 2. The foreign body after retrieval in the endoscopic suite. It appears to be a long chicken bone
Discussion
Foreign bodies in the biliary tract are a rare finding. They are mainly associated with altered biliary – enteric anatomy, most commonly presence of choledochoduodenostomy / choledochojejunostomy [1, 2]. Surgical variation of the biliary anatomy permits regurgitation of the duodenal content inside the bile duct. An especially wide BEA opening can facilitate the introduction of a sizable foreign body [1]. Moreover, a choledochoduodenostomy would probably provide easier access to a foreign body, given the linear axis connecting the pyloric sphincter with the anterior duodenal bulb. However, there have been case reports of foreign bodies even in patients with a native papilla [3]. In these patients, loss of function of the sphincteric mechanism, permitting reflux from the alimentary tract is hypothesized [3]. Patient symptoms have been attributed mainly to bouts of cholangitis [1] and formation of bile stones [3]. Foreign bodies in the biliary tract (bone, toothpick, phytobezoar) act as nidus for the formation of stones. These foreign bodies are usually amendable to common endoscopic procedures [endoscopy and possibly endoscopic retrograde cholangio – pancreatography (ERCP) [2]. Our patient did not exhibit clinical (Charcot’s triad) or laboratory (elevated liver function tests) evidence of cholangitis. Moreover, ERCP or magnetic resonance cholangio – pancreatography (MRCP) was not performed. The cause of pain might be only mechanical due to transient obstruction or distention of the opening of the bile duct or the duodenum (resulting from retrogression of the foreign body).
Conflict of interest disclosure
None
Declaration of funding sources
None
Author Contributions
Christos Konstantakis: conception and design; drafting of the article; Spyros Spyropoulos: drafting of the article. Vasileios Margaritis: drafting and critical revision of the article for important intellectual content; final approval of the article.
References
1. Yu M, Huang B, Lin Y, Nie Y, Zhou Z, Liu S, et al. Acute obstructive cholangitis due to fishbone in the common bile duct: a case report and review of the literature. BMC Gastroenterol. 2019;19(1):177.
2. Ban J L, Hirose F M, Benfield J R. Foreign bodies of the biliary tract: report of two patients and a review of the literature. Ann Surg. 1972;176(1): 102–107.
3. Cetta F, Lombardo F, Rossi S. Large Foreign Body as a Nidus for a Common Duct Stone in a Patient Without Spontaneous Biliary Enteric Fistula or Previous Abdominal Surgery. HPB Surg. 1993;6(3):235–242.