ACHAIKI IATRIKI | 2021; 40(1):49–58
Review
Anna Mastorakou1, Andreas Mastronikolis2
1BIORMONIKH O.E., Patras, Greece
2School of Physics and Astronomy, University of Manchester, UK
Received: 14 Sep 2020; Accepted: 23 Dec 2020
Corresponding author: Aikaterini Solomou, Professor of Radiology-MRI, Head og MRI Department of MR Department, Faculty of Medicine, Department of Radiology, University Hospital of Patras, 265 04, Rio- Patras, Greece, Tel.: +30 2613 603422, E-mail: solomou@med.upatras.gr
Key words: Ionizing radiation, non-ionizing radiation, radon,radiofrequency radiation, 5G.
![]()
Abstract
Radiation is part of our daily life. Exposure to low-levels of ionizing radiation does not cause immediate health effects, but can cause a small increase in the risk of cancer over a lifetime (stochastic effect), because the human body fails to repair cells and DNA mutations. Concerning non-ionizing electromagnetic radiation, epidemiological studies demonstrated an increase in childhood leukaemia associated with exposure to magnetic field above 0.3 to 0.4 µTesla. Tissue heating is the principal mechanism of interaction between radiofrequency energy, and the human body. Epidemiological studies with 15-year follow-up of individuals show a small increase in statistical risk for brain cancer (acoustic neuroma, meningioma, glioma) in the heavy use of mobile telephony, although there are potential limitations from study design and selection bias. To date, research does not suggest any consistent evidence of adverse health effects or induction of cancer from exposure to radiofrequency fields. The risks from all appliances inside homes are greater than the risks from radiation coming from a source outside the home due to the physical weakening of the exposure on a factor of distance. Analytical research states that 30cm distance from all electrical or mobile phone devices provide a lower exposure ratio. Children and pregnant women should be protected and away from potential sources of radiation.
Introduction
Online conspiracy theories linking 5G wireless services to the novel coronavirus COVID-19 outbreak had some dangerous real-world consequences. In light of recent events, the World Health Organization (WHO) and the European Commission reacted to circulating rumors and denied a possible connection between the new mobile phone generation 5G and COVID-19. WHO noted this situation as “infodemic”, namely an over-abundance of information, some accurate and some not. That makes it hard for people to find trustworthy and reliable sources when they need it. While the majority of the general public might be insensitive to conspiracy theories linking 5G to COVID-19, there are enough believers to burn down infrastructure. The only way to combat conspiracy theories is education and knowledge. The purpose of this report is to provide a summary of our current understanding of radiation risks (ionizing and non-ionizing radiation) and a synopsis of recommendations and precautions in our daily life.
Radiation
Regarding physics, radiation is the emission or transmission of energy in the form of waves or particles through space or through a material medium. The field of interest of this article is electromagnetic radiation, which is distributed in a wide spectrum of energies. Radiation is categorized as ionizing or non-ionizing depending on the energy of the emitted particles. The energy of electromagnetic radiation is determined by its frequency; ionizing radiation is high frequency and energy, whereas non-ionizing radiation is low frequency and energy. The ionizing part of the electromagnetic spectrum includes gamma rays, X-rays and the higher energy range of ultraviolet light. In the wide range of the electromagnetic spectrum, the wave energy and frequencies met on different sources tend to increase as the wavelength shortens. Frequency is expressed in Hertz (Hz), kilohertz (KHz), megahertz (MHz), gigahertz (GHz), terahertz (THz), petahertz (PHz) and exahertz (EHz). In Figure 1, the Ionizing and non-ionizing zone of electromagnetic spectrum are pictured, with frequency and wavelength analysis.

Figure 1. The electromagnetic spectrum: Ionizing and non-ionizing radiation. Different types of electromagnetic waves, frequencies, and energy bands.
Abbreviations: DC: Direct Currents; ELF: Extremely Low Frequency; VLF: Very Low Frequency; RF: Radio Frequency.
I. Ionizing radiation
It is the high-energy radiation that carries more than 10 eV, which is sufficient to remove electrons during interaction with the matter and enough to ionize atoms or molecules and break chemical bonds (directly or indirectly), leading to harmful effects on the DNA of living organisms. As stated in a review article [1] published on November 2019, DNA ionization generates direct damage to the genetic macromolecule or indirect lesions due to the formation of radicals which react inevitably with the DNA constituents. Exposure to high-energy radiation, such as x-rays, gamma rays, alpha particles, beta particles, and neutrons, can damage DNA and cause cancer. These forms of radiation can be released in accidents at nuclear power plants and atomic weapons tests or disaster.
The high energy ionizing radiation comes from natural or artificial sources. About 85% of our daily life radiation is natural and 15% artificial. 40-55% of natural radiation is due to radon. Artificial radiation refers to the radioactivity produced by medical sources, and the nuclear industry. Certain medical procedures are based upon ionizing radiation [x-rays, radiation therapy, computed tomography (CT) scans, positron emission tomography (PET) scintigraphy, etc] and can also cause cell damage that leads to cancer. However, the risks of cancer from these medical procedures are very small as compared to the benefit from having them in some medical conditions.
Expressed in Sievert (unit of measurement of the biological effect in the human body by ionizing radiation levels), the whole-body population limit exposure is 1mSv / year. Average environmental exposure to radiation is about 3mSv / year. It is crucial for public to understand the radiation protection principles of minimal time exposure, distance and shielding. The basic rule of exposure to ionizing radiation is A.L.A.R.A. (As Low As Reasonable Achievable).
I.A. Radon: The invisible threat to homes
Radon (86Rn) is the world’s most important source of exposure to ionizing radiation. Radon is a radioactive, colorless, odorless, tasteless noble gas, which is the immediate decay product of radium (226Ra), derived as a decay product of uranium (235U). The isotope 222Rn has a half-life of 3.8 days. Radon was classified as a human carcinogen in 1988, by IARC (International Agency for Research on Cancer), a branch of WHO. 222Radon is especially dangerous because it permeates soil and rocks and concentrates inside buildings and uranium mines. Radon was identified as a health problem by the fact of observed high rates of lung cancer in underground uranium miners who were exposed to it. At high concentrations, gaseous 222Rn may be inhaled and decay to radioactive polonium (210Po) in the lungs, whose high-energy alpha radiation bombards vulnerable lung tissue and damages cells. Alpha radiation is produced by alpha particles, which consist of two protons and two neutrons, structurally identical to the nucleus of the gas helium. Alpha radiation is a highly ionizing form of particle radiation with a low penetration depth that irradiates tissues, causing biological damage from chromosome alterations and mutations.
Extended periods of exposure to 222Rn and its progeny ultimately induce lung cancer, as is stated by WHO [2] and EPA (U.S. Environment Protection Agency). According to WHO, the proportion of all lung cancers linked to radon is estimated to be 3% to 14%, depending on the average radon concentration status. The majority of radon-induced lung cancers are caused by low and moderate radon concentrations. Alternatively, radon may enter the body through contaminated drinking water, making radon diffusion one of the greatest dangers of radium. Thus, 222Rn is a carcinogen; in fact, Radon is the second most important cause of lung cancer after cigarette smoking in many countries [3, 4] and in the United States, with over 20,000 deaths per year attributed to radon-induced lung cancer, according to EPA. Similar findings are found worldwide. Residential radon exposure is considered as the first cause of lung cancer in never smokers [5, 6]. Exposure to the combination of radon gas and cigarette smoke creates a greater risk of lung cancer. WHO stated that radon exposure is a major and growing public health threat in homes and recommends that countries adopt reference gas levels of 100 Bq/m3 (Becquerel per cubic meter).
Radon is a pollutant that affects the quality of indoor air worldwide. It typically moves upwards through the ground and into the house through cracks and other holes in the foundation (cracks in floors, walls, construction joints, around service pipes, etc). Radon gas enters the house being trapped inside, especially in the winter months, and in the night, when windows and doors are kept closed. It is also found in thermal springs, caves, mines, underground workplaces and well water. The Greek Atomic Energy Commission (E.E.A.E.) has much useful information about radon and an application in its website that provides access to information about radon concentrations (Bq/m3) in different regions of Greece. Measurements of the indoor radon level of a home are accomplished by request to the Commission.
I.B. Radioactive polonium: invisible threat inside tobacco
Smoke contains radioactive Polonium (210Po) with a half-life of T1/2 = 138.4 days. Polonium has been found in smoke from tobacco leaves grown with phosphate fertilizers, which contains radium (226Ra), ancestor of 210Po. 210Po is an important contaminant in the environment, mainly affecting seafood and tobacco. As a result of its intense radioactivity, it is extremely toxic to humans. During smoking, 210Po is absorbed by the bronchial system, and the lungs are exposed to alpha radiation along with other toxins, creating a toxic / carcinogenic mixture.
There are various studies confirming the radiological risk from 210Po in a smoker of 20 cigarettes per day for a year. The risk is equivalent to the one deriving from 300 chest X-rays, with an autonomous oncogenic capability of 4 lung cancers per 10.000 smokers. 210Po can also be found in passive smoke surrounding environment [7]. The U.S. International Commission on Radiation Protection (ICRP) estimates of the lifetime probability of developing lung cancer after a 1-Sv radiation dose, is 121 cases per 100 000 population (1.21%) [8].
I.C. Artificial tanning carries a risk of skin cancer
Ultraviolet radiation (UVR) is a natural part of solar radiation with wavelength from 10nm to 400nm, and is released by tanning beds, black lights, and electric arc lighting. Artificial tanning light bulbs emit UVR, which is found at the borderline zone of ionizing and non-ionizing radiation in the electromagnetic spectrum. Modern light bulbs emit ultraviolet A (UVA) and ultraviolet B (UVB) radiation, but UVA intensity can be up to 15 times stronger than solar radiation. In 2009, IARC has described ultraviolet radiation (solar and artificial), as “carcinogenic” to humans, because it causes skin cancer and melanoma. Exposure to UVR from artificial tanning beds devices leads to DNA damage in skin cells and is associated with an increased risk of developing basal / squamous cell carcinomas, and melanoma [9-11]. It has also been associated with skin burns, accelerated skin aging, ocular melanoma and immune suppression. Consistent regulation of the intensity, and UV wavelength emitted by indoor tanning devices is crucial. The use of a tanning facility in early adulthood has been strongly associated to high risk of skin cancer. Elevated vitamin D levels associated with UV exposure have been suggested to protect against various internal malignancies and other diseases, but other sources of vitamin D are easily available.
Artificial tanning devices exert their effect through the emission of both UVA and UVB radiation. While UVB is associated with direct DNA damages by the photoproducts, UVA exposure is associated with indirect DNA damages through the production of reactive oxygen species. While indoor tanning remains prevalent in population, it is clear that artificial tanning bed represents an avoidable risk for skin cancer and a widespread public health issue.
I.D. Medical diagnostic and therapeutic procedures
Even though the use of ionizing radiation in medicine poses potential risks to patients, medical personnel, and the general public, however, it also offers enormous benefits in selected cases. Modern medicine would be impossible without the use of ionizing radiation. As seen below in Table 1, radiation doses variability is high, depending on the diagnostic medical procedure.
Typical radiation doses from common medical imaging procedures
In recent decades, for dose limitation purposes, the International Commission on Radiation Protection (ICRP) has divided the diverse radiation effects into either stochastic effects (cumulative low dose effect with no apparent threshold) or tissue reactions (formerly termed non-stochastic or deterministic effects, which do have a threshold of visible injury). It is known that cancer risks increase almost linearly as exposure doses increase above approximately 150 mSv. Relying on the uncertainty of the stochastic risk from ionizing radiation associated with medical imaging, it is impossible to describe precisely the risks of a medical imaging procedure. The estimated risk from a diagnostic or therapeutic medical procedure should be compared to general statistical risks of death from other common causes.
In the late 1990s, data was released by the Radiation Effects Research Foundation of their longitudinal study of 50.000 survivors of the atomic bombs in Hiroshima and Nagasaki who were exposed to radiation doses of less than 500 mSv. Analysis of solid cancer incidence in these individuals was performed after a follow up over 55 years [12]. The investigators found direct and statically significant evidence of risk in the dose range from 50–100 mSv. Τhis linear no-threshold hypothesis is questioned by a strong biologic argument. With doses up to 50 mSv, error-free DNA repair is expected. With doses over 100 mSv, error-prone repair is possible. At this level, some aberrant cells may go on to become preneoplastic cells that may then differentiate into invasive cancers. Tubiana et al. [13] concluded there is no evidence of a carcinogenic effect for acute radiation doses less than 100 mSv. The International Atomic Energy Agency (IAEA) has adopted a protection strategy with reference level of 20-100mSv, in order to reduce the risks of stochastic effect. General principles of radiation protection from the hazard of ionizing radiation in medicine are summarized in three principles: justification of the procedure, optimization of individual protection, and dose limitation. The best approach on stochastic effects is suggested by the consensus between the physician who has the responsibility of evaluating the relevant risks from a medical procedure and the patient who has to accept those risks as possible outcomes in a written informed consent [14].
II. Non-ionizing radiation
Electromagnetic fields (EMF) are fields of energy produced by moving electrical charges. In the electromagnetic fields, the oscillations of electric and magnetic fields can propagate in space in the form of a wave and transmit energy at the speed of light. Electromagnetic radiation is defined according to its wavelength and frequency, which is defined as the number of cycles of a wave from a reference point per second. Its frequency is measured in Hz. Non-ionizing radiation sources include power lines, radio waves, microwaves, lasers, infrared radiation, and visible light. Non-ionizing electromagnetic radiation is a relatively low-energy radiation that is not able to ionize atoms or molecules but can produce kinetic energy which is converted to heat. This heat can adversely affect health in a range of ways. Non-ionizing radiation has sufficient energy for excitation (movement of an electron to a higher energy state), nerve stimulation (from 100 kHz to 10 MHz, adverse health effects (from 10MHz to 300 GHz), disturbance of the electrochemical balance of the cell membrane, and thermal effect.
Extremely low frequency (ELF) radiation is the radiation produced by structure like power lines or electrical wiring.
Radiofrequency (RF) and microwave (MV) radiation. Electromagnetic fields in the radiofrequency range are used for telecommunications applications, including cell phones, televisions, and radio transmissions. The human body absorbed energy from these devices, is estimated by a measure called the specific absorption rate (SAR), which is expressed in watts per kilogram of body weight. The effects of non-ionizing radiation depend on the intensity, frequency and degree of exposure. Although considered less dangerous than ionizing radiation, overexposure to non-ionizing radiation can cause public health issues.
II.A. Extremely low frequency (ELF) radiation
Electric fields arisen from electric charges, are measured in volts per meter (V/m). Magnetic fields arisen from the motion of electric charges are expressed in tesla (T), millitesla (mT) or microtesla (µT). Electric fields are produced independently of the device function, whereas magnetic fields are produced only when a current is flowing, and the device is functioning. Power lines produce magnetic fields continuously, due to current flowing through them. Electric fields are easily shielded or weakened by the walls, wood, metal and other objects, whereas magnetic fields can pass through buildings, living things, and most other materials. In the past years there is a public health concern and debate about daily exposure to extremely low-frequency magnetic fields (ELF-EMF) as possibly harmful to human health (cancer, neurobehavioral disturbances, etc). Pooled analyses of epidemiological studies suggested a pattern of an increase in childhood leukaemia associated with exposure to residential power magnetic field above 0.3 to 0.4 µT [15, 16]. This has resulted in the classification of ELF-EMF into category 2B, i.e., agents that are “possibly carcinogenic to humans” by the International Agency for Research on Cancer. The reference limit for electric fields set by the International Commission on Non-Ionizing Radiation Protection (ICNIRP) is 5KV/m. Exposure to electric field from home devices is far below this limit.
The overall exposure to electromagnetic radiation depends on the strength of the electromagnetic field, the distance from the source of the field, and the length of exposure time. The highest exposure occurs when there is short distance to a strong field for a long period. Table 2 shows magnetic field (μTesla) derived from different house devices depending on the distance from the source.
Typical magnetic field strength of household appliances at various distances
II.B. Radio frequency (RF)
Radiofrequency (RF) electromagnetic radiation (EMR) is the transfer of energy by radio waves. The frequency of radiofrequency electromagnetic radiation ranges from 30 kilohertz (30 kHz) to 300 gigahertz (300 GHz). Relatively high levels of exposure to RF fields can occur to workers in the broadcasting, transport, and communications industries when workplace is in proximity to RF transmitting antennas. Overall, the RF field background level from household appliances is low.
Mobile phones are low-powered radiofrequency transmitters, operating at frequencies between 450 and 2,700 MHz. The handset only transmits power when it is turned on. The power and the radiofrequency exposure fall off rapidly with the increasing distance from the handset. A person using a mobile phone 30–40 cm away from their body will have a much lower exposure to radiofrequency fields compared to the contact point. “Hands-free” devices will reduce exposure keeping mobile phones distant from the head and body during phone calls. Limiting the number and length of calls is also a best practice.
Tissue heating is the principal interaction mechanism between radiofrequency energy, and the human body. In the case of frequencies used by mobile phones, most of the energy is absorbed by the skin, and superficial tissues, resulting in negligible temperature rise in the contact point of the body. In relation to mobile phone exposure, the SAR distribution in the head depends on many factors including head size, frequency, and exposure conditions. Thus, compared to adults, higher SARs is expected to occur in children’s brain because of thinner skin, and surrounding tissue [17].
The strength of the signal transmitted between a mobile phone and base station would vary by distance between both antennas, according to the inverse square law. The use of Adaptive Power Control (APC) technique in mobile phones enables customization of output powers, so that, the signal strength and synchronization to base stations is constant and sufficient to produce good quality reception. The maximum SAR depends critically on the position of the phone and, in particular, on the distance between the antenna and the brain. Using the phone in areas of good reception also decreases exposure to the operator, as it allows cell phone to transmit at reduced power.
Several large multinational epidemiological studies have ended or are ongoing, including case-control studies and prospective cohort studies. Epidemiological studies with a 15-year follow-up of individuals show a small increase in statistical risk for brain cancer (acoustic neuroma, meningioma, glioma) in the heavy use of mobile telephony [18], although there are potential limitations from study design and selection bias.
The largest retrospective case-control study to date on adults, Interphone [18], coordinated by IARC, was designed to determine whether there are links between the use of mobile phones and brain cancers in adults. The international pooled data analysis gathered from 13 participating countries found no increased risk of glioma or meningioma with mobile phone use of more than 10 years. There are some indications of an increased risk of glioma for those who reported the highest 10% of cumulative hours of cell phone use. The researchers concluded that biases and errors limit the strength of these conclusions. Moreover, no association or possible indication between heavy mobile phone use and brain tumours, were concluded on Danish study [19], Million Women Study [20], Cerenat study [21] and Cefalo study [22]. IARC has found limited evidence that RF radiation causes cancer in animals and humans, and classified RF radiation as “possibly carcinogenic to humans” (Group 2B). This was based on the finding of a possible link in at least one study between cell phone use, and a specific type of brain tumour. IARC considers the evidence overall to be limited and inconclusive because of the methodologic limitations and conflicting findings in some studies. The U.S. Food and Drug Administration (FDA) stated that based on the current information, the current safety limits for cell phones are acceptable for protecting the public health. A large prospective cohort study of cell phone use, and its possible long-term health effects was launched in Europe in March 2010. This ongoing study, known as COSMOS, has enrolled approximately 290,000 cell phone users’ aged 18 years or older to date and will follow them for 20 to 30 years [23][24].
A number of studies have investigated the effects of radiofrequency fields on heart rate, brain electrical activity, sleep, cognitive function, and blood pressure in volunteers. To date, research does not suggest any consistent evidence of adverse health effects from exposure to radiofrequency fields. Further, research has not been able to provide support for a relationship between exposure to electromagnetic fields and self-reported symptoms of “electromagnetic hypersensitivity” [25].
II.C. Wireless local area networks
Most Wi-Fi devices operate at radiofrequencies that are broadly similar to cell phones, typically 2.4 – 2.5 GHz, although, in recent years Wi-Fi devices with higher frequencies (up to 5.8 GHz) have appeared. Radiofrequency radiation exposure from Wi-Fi devices is considerably lower than that from cell phones. Both sources emit levels of radiofrequency radiation that are far below the guideline of 10 W/m2 as specified by the ICNIRP. According to a 2019 review, there is no noticeable increase in everyday EMF exposure since 2012, despite the increasing use of wireless communication devices [26].
II.D. 5G
5G is the 5th generation of mobile networks. Due to the increased bandwidth and the higher frequency of the new network, the download speed is expected to reach up to 10 Gigabits/sec. In Figure 2, 5G band is showed in electromagnetic spectrum as compared to existing cellphones technology.
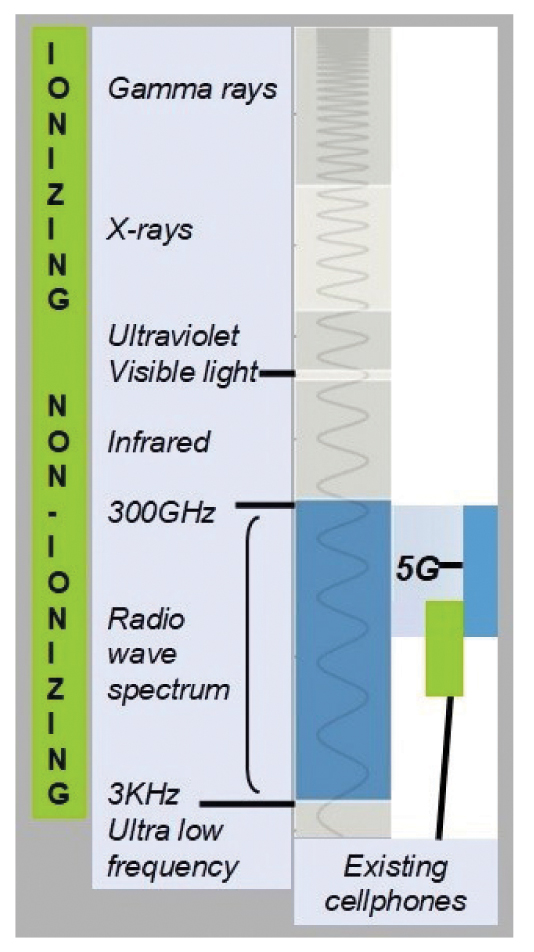
Figure 2. 5G electromagnetic spectrum. 5G operation non-ionizing band is compared to zone occupied by existing cellphones. Due to the short wavelengths, 5G does not penetrate objects and human skin, and cannot travel long distances, hence 5G technology requires a larger number of base stations than 4G.
5G technology uses millimetre waves (MMW), in addition to the microwaves that have been used to date in previous “2G, 3G, 4G” networks. The increased frequency of 5G does not necessarily mean increased user exposure, as this depends on the distance, duration of exposure and the degree of attenuation of the radiation.
Regarding physical characteristics, the non-ionizing high-frequency electromagnetic radiation of 5G has a small penetration range in the body. The skin acts as a barrier shielding the internal organs from exposure to 5G radiation. This is a fact also for sunlight and ultraviolet light which have a higher frequency than 5G. Furthermore, there is a significant weakening of 5G radiation from building materials, which explains why a denser network of base stations is required for the acquirement of stable signal.
In recent years, a growing appeal [27] from hundreds of scientists worldwide states that the increasingly extensive use of wireless technology, especially with the use of 5G technology, would expose population to constant EMF radiation because of the large number of 5G transmission stations suitable for billions of connections. In addition, the appeal points to a large number of scientific publications that illustrate EMF harmful exposure effects. They urge “the EU to follow Resolution 1815 of the Council of Europe and demand a new assessment by an independent task force”.
The 5G radio emission fields are quite different to those of previous generations because of their complex beamformed transmissions which produce a focused wireless signal towards a specific receiving device. The beam modifies vary rapidly with time and movement and so are unpredictable, as the signal levels and patterns seem to interact as a closed loop system. This has yet to be mapped reliably for real world situation, outside laboratory conditions. Along with the mode and duration of exposures, characteristics of the 5G dense signal pulse seem to increase the biologic and health impacts of exposure [28]. A 2018 review concludes that “evidence of the biological properties of radiofrequency EMF (including 5G) are accumulating progressively and preliminary studies point to the existence of multi-level interactions between high-frequency EMF and biological systems” [29].
Data from a pragmatic review that analyzed 94 relevant publications performing in vivo or in vitro investigations about the health impact of MMW, led to the conclusion that “regarding the health effects of MMW in the 6–100 GHz frequency range at power densities not exceeding the exposure guidelines the studies provide no clear evidence, due to contradictory information from the in vivo and in vitro investigations” [30].
On March 2020, the European Parliament Research Service (EPRS), by author Karaboytcheva M, issued a briefing about “Effects of 5G wireless communication on human health”. According to the 2019 European Parliament study “5G deployment: State of Play in Europe, USA and Asia”, long-term technology research is essential. One key problem is the unusual propagation phenomena, especially measuring radio frequency EMF exposure at MMW frequencies for the handset and the base station. The study states that the main problem seems to be that it is not currently possible to accurately simulate or measure 5G emissions in the real world.
In a recent statement named “Scientific Evidence for Cell Phone Safety”, FDA declared no new implications for the band of 5G maintaining the existing exposure limits and guidelines. The ICNIRP RF EMF guidelines 2020 has made a number of changes to ensure that new technologies such as 5G will not be able to cause harm. “These changes include the addition of whole-body average restrictions for frequencies >6 GHz, restrictions for brief (<6 minutes) exposures and the reduction of the averaging area for frequencies >6 GHz”. The Australian Radiation Protection and Nuclear Safety Agency (ARPANSA) stated that “the operating frequencies of the 5G network are considered within the limits and no health effects are expected from radio frequency exposures below the limits set in the ARPANSA standard”.
III. Protection and precautions instructions to public
To protect public against exposure to radon, it is necessary to check and isolate the foundation of the buildings and ventilate the interior environment so the gas escapes outside and the exposure inside the house or workplace is reduced. Radon measurement is carried out by request to the Hellenic Atomic Energy Commission. Smoking should be stopped inside home.
The full implementation of the anti-smoking law is mandatory to avoid exposure to the radioactive polonium (210Po) contained in cigarette smoke, especially in the case of passive smoking indoors. Special attention must be given to young children and pregnant women.
People should avoid exposure to artificial light devices – artificial tanning as strong exposure to ultraviolet radiation is classified as carcinogenic.
General principles of radiation protection from the hazard of ionizing radiation and the safety issues by medical radiological or nuclear medicine equipment are summarized in three principles: justification of the procedure, optimization of individual protection, and dose limit [31, 32]. In radiation therapy, the predominant issue is the avoidance of accidents.
It is recommended to restrict time using mobile phones and to remove the device far away from the user’s head and body (hands-free, Bluetooth, etc.). The safety distance must be greater than 30-40 cm [33].
In areas with bad radiofrequency signal, the exposure to operator increases, because mobile phone emits with increased power levels. It is recommended to avoid using a mobile phone in basements, enclosed spaces, elevators and on a vehicle. Metal mobile phone cover should be avoided because it leads to mobile phone operation status with maximum power.
Mobile phone should be put in flight mode whenever is possible and especially in the case of children dealing with games [33].
Schools and homes should give preference to wired internet connections and regulate strictly the use of mobile phones by the children.
The wi-fi device or other devices should not be near a bed or desk where the user’s exposure may be long. Devices that are not used at night should be turned off [33].
The use of electric blanket should be avoided during sleep. Sleeping close to iron materials is not recommended [33].
Safety distances must be kept from electrical appliances to 30 cm to weaken the exposure to electromagnetic radiation [33].
The Hellenic Atomic Energy Commission is responsible for the installation, and operation of mobile telephony and radio frequency antennas. There are annual reports for compliance to security limits, mapping of mobile phone antenna measurements nationwide and information material on the EEAE website (https://eeae.gr/).
Conflict of interest disclosure: None to declare
Declaration of funding sources: None to declare.
Author contributions: Anna Mastorakou: conception, design, drafting of the article; critical revision of the article for important intellectual content; final approval of the article and Andreas Mastronikolis: analysis and interpretation of physical data; final approval of the article.
References
-
- Mavragani IV, Nikitaki Z, Kalospyros SA, Georgakilas AG. Ionizing Radiation and Complex DNA Damage: From Prediction to Detection Challenges and Biological Significance. Cancers (Basel). 2019;11(11):1789.
- Ting D. WHO Handbook on Indoor Radon: A Public Health Perspective. International Journal of Environmental Studies. 2010;67(1):100-102.
- Darby S, Hill D, Auvinen A, Barros-Dios JM, Baysson H, Bochicchio F, et al. Radon in homes and risk of lung cancer: collaborative analysis of individual data from 13 European case-control studies. BMJ. 2005;330(7485):223.
- Gaskin J, Coyle D, Whyte J, Krewksi D. Global Estimate of Lung Cancer Mortality Attributable to Residential Radon. Environ Health Perspect. 2018;126(5):057009.
- Rodríguez-Martínez Á, Torres-Durán M, Barros-Dios JM, Ruano-Ravina A. Residential radon and small cell lung cancer. A systematic review. Cancer Letters. 2018;426:57–62.
- Torres-Durán M, Ruano-Ravina A, Parente-Lamelas I, Leiro-Fernández V, Abal-Arca J., Montero-Martínez C, et al. Residential Radon and Lung Cancer Characteristics in Never Smokers. Int J Radiat Biol. 2015;91(8):605-10.
- Zagà V, Lygidakis C, Chaouachi K, Gattavecchia E. Polonium and Lung Cancer. J Oncol. 2011; 2011:860103.
- Karagueuzian HS, White C, Sayre J, Norman A. Cigarette Smoke Radioactivity and Lung Cancer Risk. Nicotine Tob Res.2012;14(1):79-90.
- Schulman JM, Fisher DE. Indoor ultraviolet tanning and skin cancer: health risks and opportunities. Curr Opin. 2009;21(2):144–149.
- Le Clair MZ, Cockburn MG. Tanning bed use and melanoma: Establishing risk and improving prevention interventions. Prev Med Rep. 2016;3:139–144.
- Boniol M, Autier P, Boyle P, Gandini S. Cutaneous melanoma attributable to sunbed use: systematic review and meta-analysis. BMJ. 2012;345:e4757.
- Pierce DA, Preston DL. Radiation-related cancer risks at low doses among atomic bomb survivors. Radiat Res. 2000;154(2):178–186.
- Tubiana M, Feinendegen LE, Yang C, Kaminski JM. The Linear No-Threshold Relationship Is Inconsistent with Radiation Biologic and Experimental Data. Radiology. 2009;251(1):13–22.
- Brink JA, Goske MJ, Patti JA. Informed Decision Making Trumps Informed Consent for Medical Imaging with Ionizing Radiation. Radiology. 2012;262(1):11–14.
- Kheifets L, Ahlbom A, Crespi CM, Draper G, Hagihara J, Lowenthal RM, et al. Pooled analysis of recent studies on magnetic fields and childhood leukaemia. Br J Cancer.2010;103(7):1128–1135.
- Amoon AT, Crespi CM, Ahlbom A, Bhatnagar M, Bray I, Bunch KJ, et al. Proximity to overhead power lines and childhood leukaemia: an international pooled analysis. Br J Cancer. 2018;119(3):364‐373.
- Cardis E, Deltour I, Mann S, Moissonnier M, Taki M, Varsier N, et al. Distribution of RF energy emitted by mobile phones in anatomical structures of the brain. Phys Med Biol. 2008;53(11):2771‐2783.
- Swerdlow AJ, Feychting M, Green AC, Kheifets L, Savitz DA. Mobile Phones, Brain Tumors, and the Interphone Study: Where Are We Now? Environ Health Perspect. 2011;119(11):1534–1538.
- Frei P, Poulsen AH, Johansen C, Olsen JH, Steding-Jessen M, Schuz J. Use of mobile phones and risk of brain tumours: update of Danish cohort study. BMJ. 2011;343:d6387.
- Benson VS, Pirie K, Schüz J, Reeves GK, Beral V, Green J, et al. Mobile phone use and risk of brain neoplasms and other cancers: prospective study. Int J Epidemiol. 2013;42(3):792‐802.
- Coureau G, Bouvier G, Lebailly P, Fabbro-Peray P, Gruber A, Leffondre K, et al. Mobile phone use and brain tumours in the CERENAT case-control study. Occup Environ Med. 2014;71(7):514‐522.
- Aydin D, Feychting M, Schüz J, Tynes T, Andersen TV, Schmidt LS, et al. Mobile phone use and brain tumors in children and adolescents: a multicenter case-control study. J Natl Cancer Inst. 2011;103(16):1264‐1276.
- Schüz J, Elliott P, Auvinen A, Kromhout H, Poulsen AH, Johansen C, et al. An international prospective cohort study of mobile phone users and health (Cosmos): design considerations and enrolment. Cancer Epidemiol. 2011;35(1): 37‐43.
- Toledano MB, Auvinen A, Tettamanti G, Cao Y, Feychting M, Ahlborn A, et al. An international prospective cohort study of mobile phone users and health (COSMOS): Factors affecting validity of self-reported mobile phone use. Int J Hyg Environ Health. 2018;221(1):1‐8.
- (ICNIRP) Guidelines for Limiting Exposure to Electromagnetic Fields (100 kHz to 300 GHz). Health Phys. 2020;118(5):483–524.
- Jalilian H, Eeftens M, Ziaei M, & Röösli M. Public exposure to radiofrequency electromagnetic fields in everyday microenvironments: An updated systematic review for Europe. Environ Res. 2019;176:108517.
- Hardell L, Nyberg R. Appeals that matter or not on a moratorium on the deployment of the fifth generation, 5G, for microwave radiation. Mol Clin Oncol. 2020;12(3):247-257.
- Kostoff RN, Heroux P, Aschner M, Tsatsakis A. Adverse health effects of 5G mobile networking technology under real-life conditions. Toxicol Lett. 2020;323:35-40.
- Di Ciaula A. Towards 5G communication systems: Are there health implications? Int J Hyg Environ Health. 2018;221(3):367–375.
- Simkó M, Mattsson MO. 5G Wireless Communication and Health Effects—A Pragmatic Review Based on Available Studies Regarding 6 to 100 GHz. Int J Hyg Environ Health. 2019;16(18):3406.
- ICRP Publication 105. Radiation protection in medicine. Ann ICRP. 2007;37(6):1‐63.
- Do KH. General Principles of Radiation Protection in Fields of Diagnostic Medical Exposure. J Korean Med Sci. 2016;31 Suppl 1(Suppl 1):S6‐S9.
- Belyaev I, Dean A, Eger H, Hubmann G, Jandrisovits R, Kern M, et al. EUROPAEM EMF Guideline 2016 for the prevention, diagnosis and treatment of EMF-related health problems and illnesses. Rev Environ Health. 2016;31(3):363‐397.